

Dupuytren disease is genetic. It runs in families – but how? It depends on ancestry, age, gender, and relatives.

Not everyone with Dupuytren has bent fingers. Dupuytren disease is any Dupuytren changes of the palms. Nodules, puckered skin, or cords are all signs of Dupuytren disease. Dupuytren contracture is Dupuytren disease plus bent fingers. The graphic on the left represents everyone with Dupuytren. At any one time, most have no contracture – the blue people. The pink people have mild contractures that are not bent enough for a procedure. The red people are the proportion with the greatest contractures ready for a straightening procedure. Anyone with Dupuytren disease can progress from blue to pink to red.
The more severe one’s biology, the more likely it is to progress and to recur. We need an accurate way to measure an individual’s Dupuytren biology, predict their risk of progression, and test whether medicines can correct the abnormal biology. This is one of the main goals of the Dupuytren Research Group’s blood biomarker research.
You can diagnose Dupuytren by looking at the hands. What’s the point of a blood test?
Appearances only show what Dupuytren has already done to the hands, not what it will do. Appearances can’t answer questions like these: If my hands look normal now, will I develop Dupuytren? Will my children? If only my parents have Dupuytren, will my children? If I have Dupuytren but no bent fingers, will my hands worsen? If I have a procedure for bent fingers, will it last? Right now, the only answers from doctors are odds – like gambling odds. There are no precise answers for individual people. There’s no way to predict if a treatment today will change what happens over the long term. We need a blood test to answer these questions on an individual basis.
What is the baseline risk for developing Dupuytren?
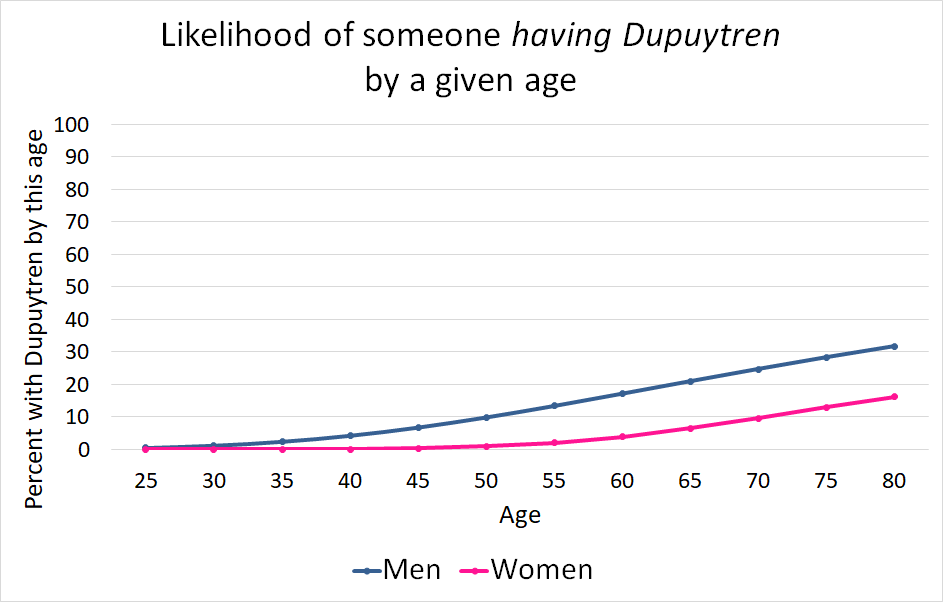
The most significant overall risk for developing Dupuytren is European ancestry. The timeline depends on age and gender. One in ten men of European ancestry will have Dupuytren by their 50s and one in four by age 70 (1). The percentage of affected women lags 15 to 20 years behind men.
Will my children inherit my Dupuytren disease?
“I have Dupuytren. What is the likelihood my children will?” The short answer is each child will have about a 50:50 chance of developing Dupuytren. Dupuytren usually develops later in life. Family trees aren’t reliable if children are young – and for Dupuytren, young means under 50. A study of Dupuytren families with children aged 50 or older concluded that if one parent had Dupuytren, each child had about a 50% chance of developing Dupuytren by age 50 or older (2).
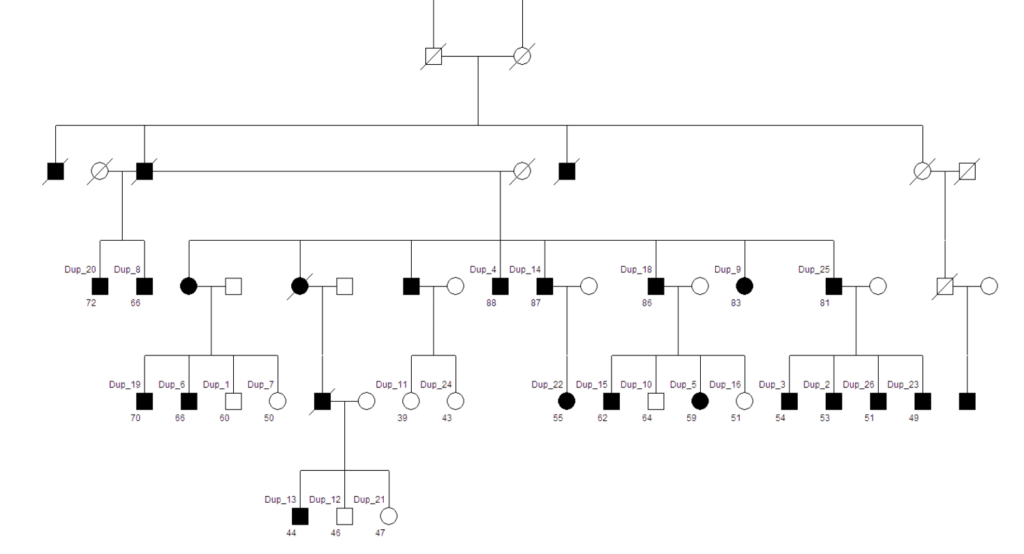
This does not mean if you have Dupuytren and have two children, one will automatically develop Dupuytren. Take a coin toss, for instance: a coin flip has 50:50 odds as well. If the first flip is heads, it doesn’t mean the next flip will be tails. The following five flips might be heads. Or tails. Dupuytren can skip several generations or can show up throughout an entire family.
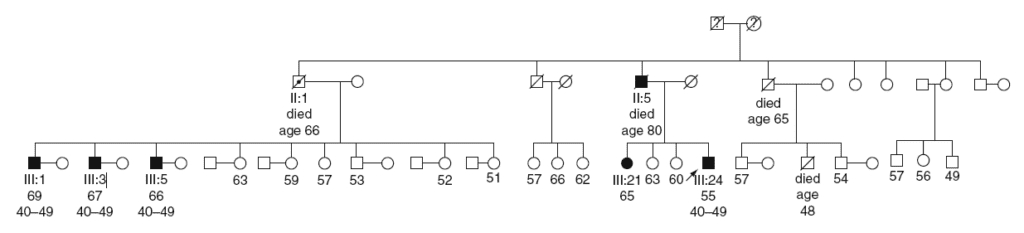
For example, in these pedigree charts shown below, family members with Dupuytren are the solid circles (women) and squares (men). In the first chart, one person with Dupuytren had no known direct ancestors with Dupuytren, going back three generations. Parents with Dupuytren genes might not develop Dupuytren themselves but can pass these genes on to their children.
Genes aren’t the only factor: one can have Dupuytren genes but never develop the condition – or live long enough to develop it. Lifestyle (smoking, drinking, heavy hand use at work or play), medical issues (diabetes), local trauma (accidental injury, surgery), and other unknown factors may also affect whether someone with the genes develops the condition. Still, studies have consistently concluded genes are the major risk factor and have a much greater effect than other factors on the risk of developing Dupuytren (4). If you have Dupuytren, each of your children has roughly a 50:50 chance of developing it – even if you developed it after they were born.
How likely is someone to develop Dupuytren if both parents have Dupuytren? The short answer is very likely. Based on current scientific evidence, if both parents have Dupuytren, each child has roughly 3:1 odds of eventually developing Dupuytren.
Will my Dupuytren affect the severity of my child’s Dupuytren? On average, yes. Analysis of the Dupuytren Research Group’s International Dupuytren Database found patients with one affected parent needed a finger-straightening procedure an average of four years younger than those with no affected parents. If both parents had Dupuytren, they averaged six years younger at their first procedure. Other researchers have also reported that if both family lines are affected, children are more likely to need treatment at a younger age (5) or have more severe biology (6, 7). People who need their first procedure at a younger age are more likely to have recurrence after treatment.
Siblings (Brothers, Sisters)
“My sibling has Dupuytren, but I don’t – yet. What is the likelihood I will develop Dupuytren during my lifetime?” The short answer is you are much more likely to develop the disease than if none of your siblings has Dupuytren. Sibling Recurrence Risk is how likely it is for a person to have the disease compared to the general population. A sibling recurrence risk of 3 means a person’s risk of having Dupuytren is three times greater than if no sibling was affected. A sibling recurrence risk of 6 means the person has six times the risk. Different studies have calculated, for Dupuytren, this number is somewhere between 3 and 6 (3, 8, 9).
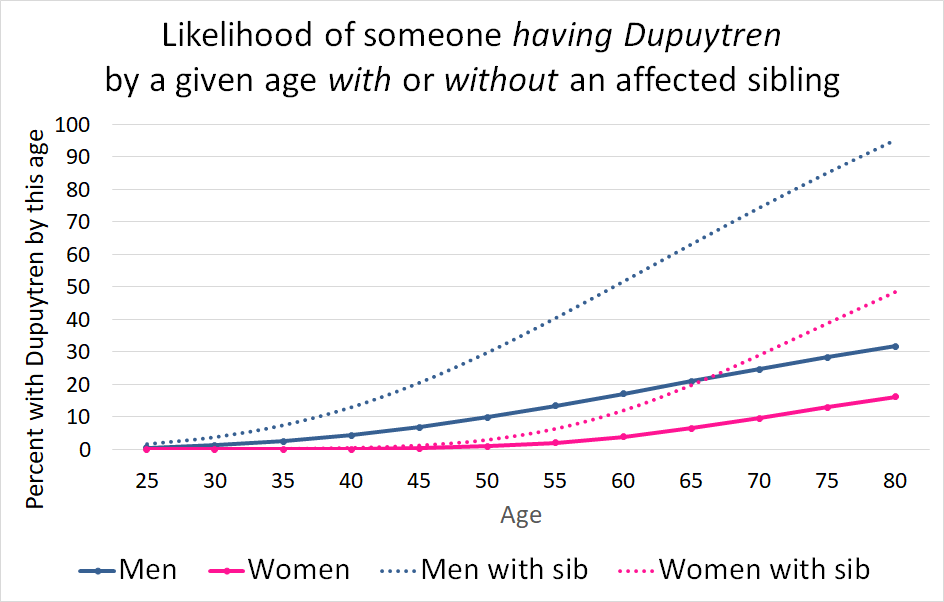
A sibling recurrence risk of 3 means having an affected sibling triples one’s disease risk. 10% of men with European ancestry have Dupuytren by their 50s, meaning a man with an affected sibling has at least a 30% (3 × 10%) chance of having Dupuytren by his 50s. Because the risk of Dupuytren increases steadily with age, that number approaches 100% for those in their 70s who have an affected sibling. On average, women develop Dupuytren later in life, so their corresponding numbers are lower, as shown in this chart.
What if my identical twin has Dupuytren? There’s no specific data available on this, but based on what is known, the answer is most likely.
Dupuytren and Ledderhose
Ledderhose disease affects the soles of the feet, usually in the instep. Its biology and demographics are similar to Dupuytren. One in five patients with Dupuytren also have Ledderhose (10, 11), suggesting Ledderhose and Dupuytren might be the same disease in different locations. Dupuytren patients with Ledderhose are more likely to have Dupuytren in their family than those without (11), pointing to a shared inheritance. Ledderhose often develops years before a person develops Dupuytren. Although there are no studies on this, Ledderhose alone is likely a risk factor for Dupuytren in future generations of the family.
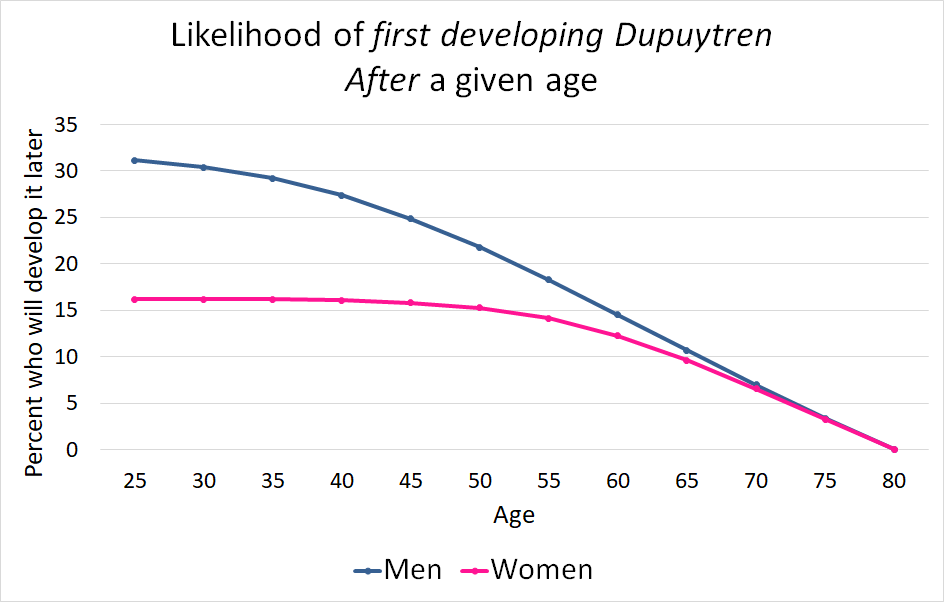
One benefit of growing old
Good news: If you haven’t developed Dupuytren yet, the older you are, the less likely it is for you to develop it.
In conclusion, Dupuytren is much more heritable than many other genetic diseases. If Dupuytren is in your family now, it will likely stay in your family until treatments that work for a lifetime are developed. Dupuytren blood test research is the key to developing a cure.
The Dupuytren Research Group is a 501(c)(3) nonprofit. We believe Dupuytren can be cured, and we are the only global organization focused entirely on this goal. Our blood test research is the key to a cure and is only possible because of our donors. Our fundraising goal for 2024 research is $250,000. Please make a difference and join our supporters to help find a cure. Invest in a future without Dupuytren disease.
– this post was updated 12/13/2023
References
- Lanting R, Broekstra DC, Werker PM, van den Heuvel ER. A systematic review and meta-analysis on the prevalence of Dupuytren disease in the general population of Western countries. Plast Reconstr Surg. 2014;133(3):593-603.
- Dolmans GHCG, Wijmenga C, Ophoff R, Werker PMN. A Clinical Genetic Study of Familial Dupuytren’s Disease in the Netherlands. Dupuytren’s Disease and Related Hyperproliferative Disorders, 2012. p. 115-22.
- Hindocha S. Identification of biomarkers and whole genome scanning in Dupuytren’s Disease. Doctor of Medicine Thesis, University of Manchester, School of Medicine, Plastic and Reconstructive Surgery Research, 2013
- Larsen S, Krogsgaard DG, Aagaard Larsen L, Iachina M, Skytthe A, Frederiksen H. Genetic and environmental influences in Dupuytren’s disease: a study of 30,330 Danish twin pairs. J Hand Surg Eur Vol. 2015;40(2):171-6.
- Becker K. Molecular Genetics of Dupuytren’s Disease. Doctoral dissertation, Faculty of Mathematics and Natural Sciences at the University of Cologne; 2012.
- Ling RS. The Genetic Factor in Dupuytren’s Disease. J Bone Joint Surg Br. 1963;45(4):709-18.
- James J. The Genetic Pattern of Dupuytren’s Contracture and Idiopathic Epilepsy. In: Hueston J, Tubiana R, editors. Dupuytren’s Disease. London: Grune & Stratton; 1974. p. 37-42.
- Hindocha S, Stanley JK, Watson S, Bayat A. Dupuytren’s diathesis revisited: Evaluation of prognostic indicators for risk of disease recurrence. J Hand Surg Am. 2006;31(10):1626-34.
- Capstick R, Bragg T, Giele H, Furniss D. Sibling recurrence risk in Dupuytren’s disease. J Hand Surg Eur Vol. 2013;38(4):424-9.
- Mohede DCJ, Riesmeijer SA, de Jong IJ, Werker PMN, van Driel MF. Prevalence of Peyronie and Ledderhose Diseases in a Series of 730 Patients with Dupuytren Disease. Plast Reconstr Surg. 2020;145(4):978-84.
- Eaton C. The Next Stage of Clinical Dupuytren Research: Biomarkers and Chronic Disease Research Tools. In: Werker PMN, Dias J, Eaton C, et al (eds). Dupuytren Disease and Related Diseases – The Cutting Edge. Switzerland: Springer; 2017. p. 391-407.




