
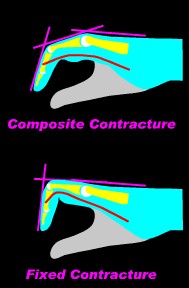
Dupuytren’s contracture is a benign condition which causes a tightening of the flesh beneath the skin of the palm and can result in permanently bent fingers. There is a sheet of tissue just under the skin of the palm which is stuck to the undersurface of the skin of the palm. This layer, called fascia, reinforces the skin of the palm. The fascia looks like cloth, and has fine threads which run lengthwise from the palm into the fingers. Dupuytren’s disease makes these lengthwise threads shrink, and they can become too short to let the fingers straighten all the way. Trying to straighten the fingers pulls the threads taut, and they feel like a string under the skin, called a cord. The taut cord holds the fingers bent like the string on a bow. The cord may feel like a tendon, but it is actually between the tendon and the skin. There are more common reasons for people to develop bent fingers, including arthritis, trigger finger, or the after effects of injury or reflex sympathetic dystrophy – but these conditions are not Dupuytren’s disease and are treated differently.
The medical definition of Dupuytren’s is a specific condition characterized by proliferation of contractile, fibroblastic cells involving the palmar fascia of the hand. It is chronic and progressive. Involved areas show microscopic inflammation, similar to that seen in wound healing and some types of cancer, as though the body were healing a deep wound beneath the skin.
The medical definition of Dupuytren’s is a specific condition characterized by proliferation of contractile, fibroblastic cells involving the palmar fascia of the hand. It is chronic and progressive 11252689 . Involved areas show microscopic inflammation 10463754, similar to that seen in wound healing 6740656 and some types of cancer 6491814, as though the body were healing a deep wound beneath the skin 10473143, 8056970.
Guillaume Dupuytren (1777-1835) was Napoleon’s surgeon, and in his time was the most famous surgeon in France. In 1831 at the Hotel-Dieu Hospital in Paris, he performed surgery and then lectured on a condition causing bent fingers, which since has borne his name. Dupuytren was not the first to describe the condition – it could just have well been called “Cooper’s Contracture”: Sir Astley Cooper published a description of the disease and its surgical treatment in England nearly 10 years before Dupuytren. Others preceded him in describing the condition, including anatomist Felix Plater 200 years earlier.
The exact process is still unknown, despite many bits of information. The body chemistry is abnormal in the entire region, even in areas not visibly changed by Dupuytren’s 3373152, 6768572, 589933, 9369955, 8501391. Here are a few parts of the picture – see if you can figure out how all of this fits together…
- The balance between certain enzymes (matrix metalloproteinases 14504511, 9768907, fibrinolysins 3958550, plasminogen activators 3693826) and their natural inhibitors is disturbed in patients with active Dupuytren’s disease, and may be affected by tension on the affected tissues 9665512.
- The cells in the cords of Dupuytren’s disease are unusually sensitive to the effects of “growth factors”, normal body chemicals involved in wound healing. These include transforming growth factor beta 1 (TGF-beta(1) 12849947, 12729127 ,8618012, transforming growth factor beta 2 (TGF-beta(2) 12678125, 8683048, basic fibroblast growth factor (bFGF)1325742, platelet derived growth factor (PDGF) 12087679, 7822340, 1564283 and others 9120728, 7722248, 8056971,8320323. The process may be triggered by a combination of mechanical stress and either TGF-beta 10050239, or PDGF8893764 .
- Dupuytren’s cords have unusually high levels of levels of the protein tyrosine phosphorylated beta-catenin 12802275 , and the cells have higher than normal levels of the substance alpha smooth muscle actin 11599921 and the enzyme lysyl oxydase 6130030.
- Cell-matrix interaction abnormalities, stimulating contraction 9369955, 9065582, 8525780. A three dimensional mesh of actin microfilaments (the “fibronexus”) links cells to each other and to the extracellular matrix 1867394, which, in Dupuytren’s disease, contains unusually high levels of fibronectin 3519746, 6386626.
- Abnormal androgen receptors have been implicated in the abnormal tissue 11853085 , 10194020, 1798252, although not by all investigators 3794501.
- Low oxygen levels resulting in reactive forms of oxygen (superoxide free radicals, oxygen free radicals) due to poor circulation have been implicated 12087679, 10050241, 1769989, possibly due to activation of the enzyme xanthine oxidase1695516, 2825907. The blood clotting system may be triggered by production of high level of plasminogen activator6197420. Microvascular circulatory changes develop, with narrowing and blockage of capillaries 1960491, 2322211,2722922, microscopic hemorrhage 6693745 and other changes in the blood vessel walls 4082789, 6150573. This might explain the relationship of smoking to Dupuytren’s. Miroculatory changes may arise from abnormal regulatory nerves in the fascia itself 2472714. Nodules show near complete absence of blood vessels 6693745, and other studies show evidence of low oxygen levels in the diseased tissues 6877040.
- T-cell and B-cell Immune mechanisms , 9888668, 8099992, autoantibodies to collagen 8181183, 3485693 or other immune mechanisms 2471021, 3138883, 6353806 may be involved.
- Genetic variations have been demonstrated in nodules, in the form of recurrent clonal numerical abnormalities 9973941,9352799,3414684.
- The contraction is due to a mechanism also seen in other contracting tissues such as healing wounds and some types of cancers 6491814. Dupuytren’s fibroblasts 6507097 can acquire smooth muscle characteristics and are then able to contract 7642925. These modified fibroblasts are called myofibroblasts 1960491, and are found in nodules, but not cords1769990, 6491814, 7071229. In diffuse disease, these changes can affect cells in the skin as well as the fascia 8294839. Myofibroblasts contract through an interaction of myofilaments and the enzyme ATPase within their cell bodies, and the extent of recurrence after surgery correlates with myofibroblast activity at the time of surgery 6683733, 2754197.
- Certain nerve endings (Pacinian corpuscles) are enlarged and surrounded by fibrous tissue in affected areas 3358315,2472714.
- Overall collagen metabolism may be disturbed in patients with Dupuytren’s 2883783. Type III collagen is increased in Dupuytren’s cords 6386626, 6740656.
- Mechanical tension forces or stretching the affected area may provoke contracture 14599823, 12866952, 12449347,10050239, 9763277, 9665511, possibly by stimulating changes in the microcirculation 8917718. Dynamic physical forces may produce biochemical changes through changes in tissue electrical fields 1284015 . Paradoxically, continuous tension on the tissues causes a temporary reversal of the process, probably by stimulating enzymes involved in tissue remodelling7964107. One hypothesis is that loss of normal gliding motion between layers of fascia results in abnormal tissue tension which provokes the contracture process 7152372.
Dupuytren disease has been referred to as a Viking or Celtic disease, but existed in Europe earlier than the Viking Age8345270 and originated much earlier in prehistory 12015711 . James Barrie, author of “Peter Pan” had a right contracture thought to be Dupuytren’s, which formed the source material for Captain Hook’s hook. The Papal Benediction sign, with bent ring and small fingers, may have started with a pope with the condition 10050238.
Depends on the genetic makeup of the population. Dupuytren is estimated to affect 3% of the US population 2190416.
 The disease process includes two structures, the nodule and the cord, which are quite different microscopically and biochemically 3351230, 12849947, 12087679, 12087251,11599921, 9665511, 7594997, 3138883, 6491814, and early (“proliferative”) nodules are biologically different from mature (“involutional”) nodules 3958550, 6150573. Dupuytren’s nodules represent the early, active form of fibrosis, and are the hard lumps in the palm. Cords develop later; they feel like strings beneath the skin and are responsible for the tethering which results in contractures.
The disease process includes two structures, the nodule and the cord, which are quite different microscopically and biochemically 3351230, 12849947, 12087679, 12087251,11599921, 9665511, 7594997, 3138883, 6491814, and early (“proliferative”) nodules are biologically different from mature (“involutional”) nodules 3958550, 6150573. Dupuytren’s nodules represent the early, active form of fibrosis, and are the hard lumps in the palm. Cords develop later; they feel like strings beneath the skin and are responsible for the tethering which results in contractures.
Dupuytren is a change in normal structures 6099177, transforming the superficial palmar fascia into cords, and joins fascia to the undersurface of the skin to form nodules 7071229. Although resembling a tumor in some ways 6197420, it is not. The longitudinal (lengthwise) fibers of the superficial palmar fascia are clinically affected 3068887, but transverse (sideways) fibers also show chromosomal evidence of involvement 3414684. Although only certain regions of the fascia appear affected, the biochemistry of the entire fascia is abnormal 6197420. The ring finger is most commonly affected, then the small finger, and then the thumb (28%) 12531665. Thumb involvement can take many forms 3958553, 7049485, and usually occurs when other fingers are affected 10050250. Rarely, the wrist may be involved 11901473, 9119844 , 8771479. “Knuckle pads” 3190317,2943155 on the dorsal PIP joints are apparently the same process as nodules in the palm. Although neither produce contractures 6707508, knuckle pads are associated with more aggressive forms of the disease 1960491. Isolated cords in the fingers may develop between the proximal phalanx periosteum (bone lining at the base of the finger) and the flexor tendon sheath at the middle phalanx level 3968392. Abductor pollicis muscle and tendon involvement may affect small finger contractures 6512361.
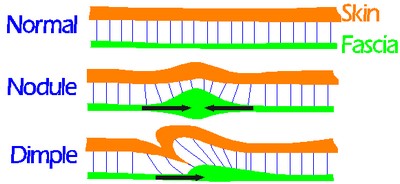
Normally, the skin is anchored down to the underlying fascia by many tiny tissue strands running perpendicular down to the fascia. When the fascia shrinks, these threads pull the skin, and may result in nodules, dimples, or both contour changes:
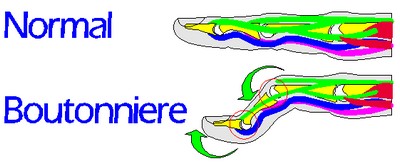
Secondary changes may also occur. The position of the finger nerves may be shifted by the growth of a “spiral cord”, especially when the PIP joints become contracted 7822934, 1769988. Extensor tendons on the back of the finger may be indirectly affected4015238: the central slip tendon which straightens the PIP joint may become stretched out from the joint being bent for a long time 7806815, and the transverse retinacular ligaments on the sides of the joint may become fibrotic, resulting in a boutonniere deformity 3249131, 3190317.
Rarely, the extensor tendons may be affected by PIP knuckle pads 6693470 or distal to the PIP joint 7119399. Other changes in the PIP joint may prevent full correction of contracture 4078465 using surgical techniques which work for non-Dupuytren’s PIP contractures 1779164. Bone spurs may develop in the finger bones as a result of tension on the attachments to bones11982519, 10433443. Rarely, the DIP joints are involved 1773223.
Outside the hand, the sole of the foot (Ledderhose’s disease) and the penis (Peyronie’s Disease) may be affected in a similar fashion. The combination of all three conditions – Dupuytren’s diathesis, Ledderhose’s contracture and Peyronie’s disease – is referred to as Dupuytren’s diathesis 8817754 and is associated with a particularly aggressive condition.
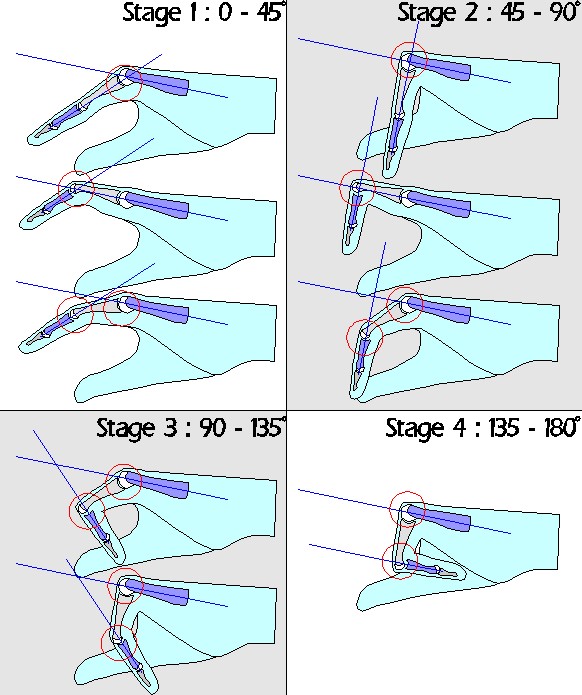
The disease often causes progressive contractures. Involved tissues become fibrous and rarely may develop cartilage or calcium deposits. The younger the person is when they first develop Dupuytren’s, the more likely they will need surgery, and the younger the patient is when surgery is needed, the greater the chance for recurrence. Overall, finger contractures develop in about one in 20 people with Dupuytren’s disease. If finger contractures develop, eventually, function is lost – but function and dexterity can be improved with correction of the contractures. Spontaneous regression is rare. Spontaneous regression of knuckle pads has been reported in children.
| RISK FACTOR | AVAILABLE DATA |
| Genes | Dupuytren’s disease is most common in white males of Northern European descent 1810624, 10050242. It is uncommon in blacks 11770364, 9665514, 8074370, and in blacks is more often associated with a history of trauma 8891992. A US Veterans study gave this racial breakdown: the incidence of Dupuytren’s in their study was Caucasian: 0.7%; Hispanic: 0.2%; Black: 0.1%; Native American: 0.1%; Asian: 0.07% 10883614. Dupuytren’s is six times more common in men than women 10883614, 10473157. Women develop the disease on the average ten years later than men 11357696, 10473157. The disease appears to run in families, and often follows an autosomal dominant inheritance 10050243. Dupuytren’s contracture has been reported in in 21% of women and 39% of men over the age of 60 in North-east Scotland. 8501390. Even with a genetic predisposition, presentation is variable, and identical twins with Dupuytrens do not necessarily have identical disease 8345271. There are genetic differences between patients with and without Dupuytren’s 12794452, 12783014 , 11924651. Although a genetic pattern of HLA DR antigens has been reported in both Dupuytren’s and scleroderma 6334711, a “Dupuytren’s gene” has not been identified 11895345. |
| Age | Increasing age increases the risk of developing Dupuytren’s 3592873. Although reported in infants 11418917,3924790 children 12703034 , 11912542 and teenagers 8676015 , this is rare. Other childhood conditions11117052 may mimic Dupuytren’s, such as the benign recurring digital fibroma of childhood or malignant epithelioid sarcoma 11912542, 10612139, 7719607. In Iceland, where it is common, Dupuytren’s in men found in 7% in the age group 45-49 years, 40% in those 70-74 years old 10760640. In Norway, 30% of the population over 60 has Dupuytren’s 10050243. |
| Diabetes | There is a five 7713273 to ten 9382632 times increased risk for diabetics to develop Dupuytren’s contracture8697659, 7722249, 10883614, 2522373, 10760640, related to the duration 3590817, 6343018, presence of diabetic retinopathy 6343018, but not severity of the diabetes 6608923, 6343018, 9002027, 2725939. In diabetics, Dupuytren’s is often a less aggressive form, but the radial hand is more often involved 6725338. |
| Diabetic Limited Joint Mobility Syndrome | Patients with this are twice as likely to have Dupuytren’s than with diabetes alone 2057690, 2522373, 6608923,2968881, and relates to the duration of diabetes 4042798. The relationship may be explained by smoking, which predisposes to both conditions 2022177, 2522859 |
| Smoking | Smokers have increased risk 9119843, 10883614, 2022177, 2522859, 3592873, 10760640, 10760640. Twice the risk of nonsmokers 3225413 |
| Alcoholism | Increased 2871816, 10883614, although some surveys dispute this 8426337, 11697563 The association may instead be with smoking 9119843 or hyperlipidemia associated with alcoholism 1447259, or alcoholic liver disease 7224858, 190684. Alcoholic liver disease is a risk factor, nonalcoholic liver disease is not 3592873, although this is also disputed 6672504. |
| Thyroid disorders | Increased incidence, more for hypothyroidism than hyperthyroidism 12864792 |
| Stretching | Contrary to natural instinct, the act of stretching the skin of the palm appears to aggravate or provoke Dupuytren’s contracture 6884845. |
| Frozen Shoulder | 50% chance of developing Dupuytren’s 11307078, 10509873, even more common with diabetes 10509873 |
| Peyronie’s Disease | 15 – 25% incidence 7150935, 9636000, 8976282, 80% in familial forms of Peyronie’s 6980996. |
| Ledderhose Disease | 28% chance of having Dupuytren’s 10919621 |
| Rheumatoid Arthritis | Lower chance of developing Dupuytren’s 10568426, 6747420, but when present, requires special surgical planning 3336640 |
| Trauma | Dupuytren’s may develop after hand trauma 3592873, 3744141, 4031627, particularly after Colles’ wrist fracture (distal radius fracture) 3998585, 9382639, 1588210. One study reported a 40% incidence of Dupuytrens 18 months after Colles’ fracture 10372776. Duputren’s developing after surgery has also been reported 8856538. |
| Hyperlipidemia | Increased 1447259 |
| Vibration exposure | Increased with vibration exposure 8732927, Patients with vibration white finger syndrome two times as likely to have Dupuytren’s 1345125 |
| Epilepsy | When present, Dupuytrens appears to have a more aggressive character 1588209, although conflicting reports exist 932769. Association may be due to phenobarbitone medication rather than epilepsy itself 932769,10751924 , although this is debatable as well 1588209. There may be an association between Dupuytren’s, RSD and antiepileptic drugs 8156963, 2691374. |
| Gout | No effect 1588208. |
| Glucosamine / Chondroitin Sulfate | Glucosamine / Chondroitin sulfate preparations are available as nutritional suppliments with claims of improving joint function. Although no cause and effect relationship has been established, chondroitin sulfate 9517845,2493650, 6489852 and glycosaminoglycan 6854215 levels are elevated in the tissues affected by Dupuytren’s contracture. |
| Growth hormone therapy | Possibly 8101283 |
| Arcus senilis | Increased incidence, possibly due to mutual association with hyperlipidemia 1280972 |
| Reflex Sympathetic Dystrophy | RSD after wrist fracture triples the risk of developing Dupuytren’s compared to no RSD 10372776. There may be an association between Dupuytren’s, RSD and antiepileptic drugs 8156963 . More common postop in women2229974 and possibly related to psychological factors 1692417. There may be an association between Dupuytren’s, thoracic outlet fibrosis and reflex sympathetic dystrophy 2707653 |
| Hemodialysis | Increased, although many factors may be at play 3113084 |
| Palmaris longus | Increased risk if this tendon is present in the wrist 3794480. Excision of the palmaris longus tendon has been reported to reduce recurrence 3740784 |
| Increased serum IgA | Increased risk 6672504, 6353806 |
| Vascular insufficiency | Increased risk 8501389 |
| Manual Labor | Increased risk 10760640, 9382639, although controversial 10050242, 8732927, 1834729. Vibration exposure is a risk factor 8732927, 8672800, 1345125 |
| Carpal tunnel syndrome | Although postoperative flare has been reported as more common with simultaneous fasciectomy and carpal tunnel release 7430596, contrary reports exist 2061659. |
| Vinyl Chloride | HLA DR antigens have been identified both in Dupuytren’s patients and in patients with vinyl chloride exposure related scleroderma 6334711. An increased incidence of Dupuytren’s was reported at a polyvinyl chloride (PVC) manufacturing plant in workers who extensively handled the product 7066227. |
| HIV infection | Increased risk debated 10050242 |
| Condition | If Dupuytren’s is present, the risk for this is... |
| Diabetes | Increased 7012682, 605747, 6725338. |
| Hyperlipidemia | Increased: present over half the time 1280972 |
| Psychological problems | No association 8583880 |
| Malignancy | Increased sarcoma 11895346 , cancer 11781116, possibly due to mutual association with smoking and alcohol abuse 10961556. |
| Mortality | Increased, especially when presenting under 60 years old 10597922, 11781116 |
| Ulnar neuropathy | Increased 186961 |
| Cold induced vasospasm | Increased 186961 |
| Thin (low triceps skin fold thickness) | More likely to be thin 8501389 ? associated with smoking |
MEDICAL / ENGLISH TRANSLATIONS relating to Dupuytren’s Disease
- Aponeurosis same as Fascia.
- Aponeurectomy same as Fasciectomy.
- Aponeurotomy same as Fasciotomy.
- Aponevrosis same as Fascia (French spelling).
- Aponevrotomy same as Fasciotomy (French spelling).
- Closed two meanings: (see open)
- A procedure performed without any cut in the skin, as in a joint manipulation.
- At the end of surgery, a wound can be “closed” by sewing the skin edges together or covering the area with a skin graft or skin flap.
- Dermofasciectomy removing fascia and the overlying affected skin. This requires closing the wound with a skin graft or flap.
- DIP Distal Interphalangeal Joint. The end joint of a finger.
- Extension two meanings:
- After surgery, Dupuytren’s showing up adjacent to the area previously treated, technically different than recurrence.
- Fascia a normal reinforcing layer of tissue, found in many areas of the body. In discussions of Dupuytren’s, the fascia refers to the superficial palmar fascia, which is a clothlike layer of tissue beneath the skin of the palm, attached to the undersurface of the skin above it and the bones and muscle coverings below it. The fascia normally functions in a very similar manner to what is referred to in the garment industry as “interfacing”: a layer of stiff cloth inside clothing which maintains the clothing’s shape (interfacing and fascia share the same Latin root). The superficial palmar fascia normally acts as a scaffolding which anchors palm skin to the bones in the hand so the skin doesn’t slide around while when we grip, hold, and twist things in our hands – it maintains the shape of the skin. The fascia is a normally unnoticeable layer, not a moving part, and not the tendons which we use to move our fingers. In Dupuytren’s disease, it is the fascia which shrinks and thickens, pulling on the skin, pulling and bending the fingers. In the US, insurance companies use the term fascia, not aponeurosis.
- Fasciectomy surgery to remove the fascia. Don’t you need the fascia? Well, yes, but after fasciectomy, the body replaces what has been removed with a layer of scar tissue, which usually works well.
- Fasciotomy cutting but not removing the fascia. This refers to cutting across tight bands of fascia, letting the edges gape apart and heal back at or closer to their natural length to restore the area’s original flexibility.
- Hematoma blood clot. After surgery, if much blood collects beneath the skin or beneath a skin graft, it may result in necrosis,or a wound where there should be skin. This slows recovery but is not the same thing or danger as a blood clot in the legs (DVT) after surgery.
- Longitudinal lengthwise, as for a line drawn along the length of a finger, base to tip.
- Necrosis dead skin. If the circulation isn’t good enough to an area of skin, after a week or so, that area of skin will turn black and hard and eventually either fall off or need to be trimmed off. This can happen after surgery, usually at the edges of a cut, where it is referred to as marginal necrosis.
- Open two meanings (see closed)
- Surgically, open means regular surgery, where the skin is “opened” with a cut, as in fasciectomy. A wound which can be stitched back together. Not percutaneous.
- After surgery, when the wound is literally left open, not stitched back together. Sounds gruesome, but it really isn’t. This is what is done with the “open palm” surgical technique for Dupuytren’s
- Patient You.
- Percutaneous A procedure performed through a small puncture wound, using a needle, narrow knife or scope, no stitches.
- PIP Proximal Interphalangeal joint, the middle joint in a finger.
- Recurrence After surgery, Dupuytren’s showing up in the area previously treated, technically different than extension.
- Suture stitches
- Transverse side to side, usually refers to a sideways cut in the palm used for fasciectomy



